
California’s anti-caste discrimination bill could lead to humanity’s health equity
-
Dignity Post

- 22-09-2023 09:51
.jpg)
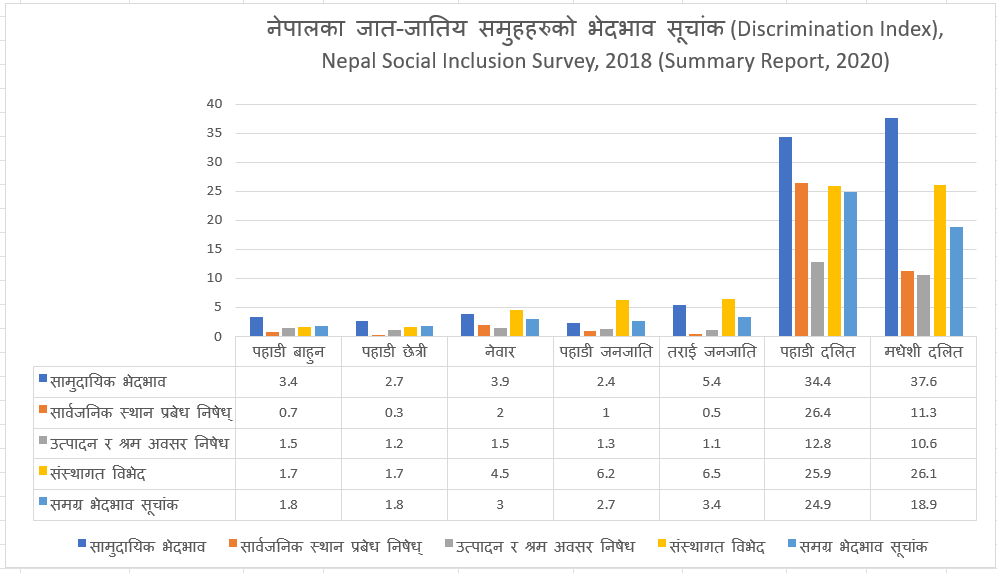
Figure 1: A spectrum of heath disparities showing caste discrimination in Nepal (Source: NDHS Nepal Report, 2006)
Dr. Drona Prakash Rasali
The California State Senate recently passed a bill to ban caste discrimination with an overwhelming 34-1 majority vote. This bill is both just and urgent, aiming to prevent a South Asian historical caste discrimination issue from taking root in American society, which already grapples with existing color-coded racism.
California Governor Gavin Newsom, who is set to evaluate the bill, is expected to sign it, weighing its alignment with the 13th Amendment of the US Constitution and the UN Universal Declaration of Human Rights.
Once this Californian bill becomes law, it will make California the third jurisdiction to ban caste-based discrimination after India and Nepal. Many other US states and local governments are likely to follow suit, as exemplified by the Seattle City Council passing a similar law last February. Educational institutions such as California State University System, Brandeis University, Brown University in the US, and the Toronto school board in Canada have also added caste to their anti-discrimination policy.
Author Isabel Wilkerson’s 2020 book, “Caste: The Origins of Our Discontents,” highlighted a lesser-known fact. In 1959, after Dr. Martin Luther King Jr. visited India, where he was introduced as a distinguished “untouchable guest from America”, he realized and declared that caste and race were equivalent in their intent to dehumanize and marginalize people in the weaker segments of society based on descent.
Recent anthropological and genomic research indicates that race and caste share common roots, stemming from the migration of Middle Eastern farmers and Great Steppe pastoralists to ancient India and Europe around 4,000 years ago. In ancient India, what is now in South Asia, the ancient migrants, later known as “Aryans”, introduced agriculture yielding surplus values. Especially, after the decline of the vibrant Indus Valley Civilization, the accumulation and distribution pattern of this surplus developed into a hierarchical caste system driven by the concentration of resources within dominant groups. Eventually, it took a cultural and religious turn due to the feudal mindset of the dominant group possessing power and privileges to control resources in the society.
Caste discrimination in ancient India, now South Asia, aimed to maintain endogamy for ancestral “purity.” However, genetic research has shown that India’s population today comprises an admixture of three sources of ancient human ancestries, in contrast to the notion of “purity”. Harvard University Genetics Professor David Reich’s team divided the Indian populations into two major clusters, Ancestral North Indians (ANI) and Ancestral South Indians (ASI). Both these clusters possess the admixture ancestries of both the ancient migrants and the Indigenous Dravidians, in a gradient of their varying proportions.
Some dissenting voices have emerged against the ban on caste discrimination in the United States. However, such arguments are unfounded in the 21st century, where discrimination based on any factor, be it race, caste, gender, age, creed, or religion, is universally considered wrong and unacceptable.
Concerns about religious sensitivity are also misplaced, as caste discrimination has now been pervasive in South Asian societies, affecting not only Hindus but also other major religious groups and Indigenous tribal communities. This discrimination gained prominence through Anglo-Hindu Law based on colonial interpretations of Hindu scriptures and customary law in British India in 1772 and the promulgation of a Civil Code in Nepal in 1854. However, none of the original Sanatan Dharma of Hindus, Buddhist Dhamma, Christianity, Islam, and Indigenous Tribal norms originally had any provision for practicing discrimination based on descent. It was only the historical feudal mindset that inculcated the notion and the practice of continuing caste-based discrimination in all these groups of populations from the Middle Ages to even today.
Caste-based discrimination negatively impacts the health and well-being of individuals and society as a whole. It perpetuates the idea of one group being superior to another by birth, leading to suffering for victims of lifelong discrimination. This occurs not only between castes but also within sub-castes. Even the Brahmins, traditionally seen as the highest caste, have several sub-castes that practice subtle discrimination by avoiding intermarriage. The most severe impact of caste discrimination is on the over 260 million Dalits in South Asia, who are forced to continue living with compromised human dignity in the 21st century. The research evidence has shown that the phenomenon of caste, or racial, discrimination has been a structural determinant of health, resulting systemically in discernible socio-economic and material deprivation of the discriminated people. These rampant health disparities have been reported in health care and health outcomes with unjust and preventable disproportionate rates of diseases across the caste groups. The whole spectrum of disadvantaged rates of health outcomes reported among Hill and Terai/Medhesh Dalits compared to other caste/ethnic identity groups in Nepal (see Figure 1) cannot be random occurrences but can be attributed to their reported high level of socio-economic discrimination indices. An analysis using India’s Annual Health Survey data reported the life expectancy of so-called upper caste Hindus at least three years higher than that of Dalits, which could not be explained by wealth or environmental exposures but was rooted in caste discrimination as a structural determinant of health.
To achieve health equity at the societal level, the elimination of racism and caste discrimination is essential. Social change occurs when constitutional and legislative measures are put in place, prompting people to not only comply with them but also change their behaviors leading to ensure equitable health and well-being for all humanity around the world.
The author is the 2023 Fulbright Canada Research Chair in Race and Health Policy at the Cecil C. Humphreys School of Law, University of Memphis, Tennessee, and an Adjunct Professor at the School of Population and Public Health, University of British Columbia, Canada. He can be reached at: dprasali@memphis.edu.






{kind=link}
Conversation